How Is 'Sanity' Different From 'Insanity'?

Featured image: The concept of 'normal' or 'typical' behaviour in the mosaic of humanity is ever-changing, vague and context-dependent. In view of this, it may not be possible to define 'abnormal' in a clinically objective way. (Naoto Hattori)
Before we had internal medicine, we had ointments, herbs and blood-letting. Before we had psychiatry, we had magic, prayers and exorcisms. Mental health vocabulary over the years has expanded, the collections of diagnoses have become extensive and the importance of mental health has reached everyday discourse. Mental illnesses have existed since the dawn of human complexity but the field of psychiatry, the branch of medicine which studies pathologies of the mind, is still fuzzy, imprecise, experimental, abundant in hypotheses and lacking in concreteness.
Underlying definitions of good mental health are assumptions about ‘right’ ways for the mind to function.
The obvious problem for psychiatry is that ‘normality’ is difficult, or even impossible, to define. Is normality an absence of mental illness? Is it happiness as emphasised by Democritus’ hedonism? Is it self-actualisation as emphasised by Aristotle’s eudaimonia? Is it the ability to function in line with societal expectation without causing harm to ourselves and others? When are we behaving like ourselves, and when are we behaving like we’re not quite ourselves? And does who we are change if we become mentally ill?
Mental health definitions are heavily influenced by their context and culture, which change over time. A definition of health which is fluid between cultures and ages is, however, a highly counterintuitive concept. What can we learn from this?
Symptomatology

Melancholy and hysteria were some of the first mental illnesses described in writing, with records dating back to Mesopotamia and Egypt. The go-to treatment for sufferers of mental illnesses was a surgical intervention: trepanning, where a small hole was drilled into the sufferer's skull to release the evil spirits causing their unrest. This practice was widespread and persisted for millennia. (Science Source)
Psychiatry is, within the context of medical sciences, an entirely unique branch. While medicine usually relates physical abnormality (e.g. infection) with symptoms (e.g. swelling and pain), psychiatric criteria for diagnosis relies on behaviour and observable data alone—physical abnormality need not be present (though it can be) and it isn’t always sought. In this way, psychiatric study of mental health is in line with the mind-body dualism as purported by René Descartes: the mind is treated as non-physical and separate from the body.
Diagnostic criteria for what constitutes psychiatric illness, and the list of mental health diagnoses, are held in two primary collections: the International Classification of Diseases (ICD) (kept and maintained by World Health Organisation) and The Diagnostic and Statistical Manual of Mental Disorders (DSM) (kept and maintained by American Psychiatric Association). Over decades, the list of disorders has been amended, changed, clarified and expanded.
Many symptoms described within the pages of both of these collections are non-specific with significant overlap and wide allowance for variability. What is and what is not considered pathological depends on the context. Additionally, these collections incorporate mental illnesses, mental disorders and neurodevelopmental disorders, not all of which are necessarily pathological in origin or warrant psychiatric intervention.
A term increasingly commonly used to describe people who do not suffer any diagnosable conditions listed in ICD and DSM is ‘neurotypical’. It originates in the autism community, used to denote individuals who are not autistic. This has become an umbrella term opposed to ‘neurodivergent’, which denotes a difference in neuronal functioning from what is considered ‘typical’. The neurodiversity movement attempts to divorce different ways of being from the idea that interventions are needed when one’s mental development or functioning is different from what is most common: de-pathologising the variability in human behaviour, learning and functioning.
But this approach fails to concretely discern what typical functioning is (and it does not aim to do so). As Ivy McKenzie stated, quoted by Oliver Sacks in The Man Who Mistook His Wife for a Hat:
Let us take dyslexia as an example to illustrate what I mean: in both ICD and DSM, dyslexia, a disorder of reading and writing with preserved intelligence, falls under ‘specific learning disorder’. However, this disorder will affect an individual more in some languages (e.g. English, where spelling is non-phonetic) than others (e.g. Serbian, where spelling is entirely phonetic). It is also more commonly diagnosed in men, although it is thought the incidence rate between the sexes is actually the same. Does this mean that in a given individual dyslexic processing of phonological data is atypical in English but typical in Serbian? Does it also mean that if the individual is female, their dyslexia is less atypical than if they were male?
The borders between health and illness, normality and abnormality, balance and imbalance, order and disorder and function and dysfunction are vague and contingent on properties of people not written into the definitions. Obsessive compulsive disorder (OCD) makes an excellent example here. OCD is defined in DSM as an anxiety disorder characterised by the presence of obsessions (recurrent intrusive thoughts) and compulsions (repetitive behaviour performed in response to an obsession). OCD is different from obsessive compulsive personality disorder, which is characterised by preoccupation with orderliness and perfectionism and control over situations. However, in terms of behaviour, both can manifest in similar ways, and the term ‘OCD’ is commonly applied in inappropriate situations (e.g. ‘I’m a bit OCD about my kitchen.’). At what point does one being tidy, neat and organised become pathological? At what point does one’s preference or need to not delegate tasks show dysfunction? And at what point is a person so overwhelmed by this way of thinking or being that psychiatric intervention is needed? These behaviours can be detrimental to both the individual expressing them as well as those they maintain relationships with: but at what point are they diagnosable?
There are limitations to what we can observe. It would seem our definitions of normality are deeply rooted in language, mode of expression and societal functioning and expectation.
The brain is not a kidney
Coordinated movement, not spasm or twitching, but dancing! took over several towns in the 1500s in Europe, a phenomenon called 'the dancing plague'. Medical historians agree now that these were most likely episodes of mass hysteria, also known as mass psychogenic illness or collective obsessional behaviour, where large groups of people partake in a common delusion. During these plagues of dancing, individuals believed they could not stop dancing due to an infectious illness that spread between them. The image above is a modernised re-imagining of Pieter Brueghel the Elder's painting The Fight Between Carnival and Lent, hypothesising what a modern-day dancing plague would look like. (Diego Agulló and Jorge Ruiz Abánades)
Mental illness is not always readily available for examination. There may be no wound, no insult, no injury, no microorganism to eradicate, or no muscle to regrow—yet its effects can be systemic and physical, from pain to a complete surrender of free will. Some examples of physical symptoms caused by mental illness include broken heart syndrome, panic attacks, and actions utterly uncharacteristic of an individual’s usual behaviour (e.g. Van Gogh amputating his own ear in a moment of ‘madness’ and ‘the devil made me do it’ legal defence). This shows (against Descartes’ theories) that the brain and body are tightly connected, evidenced by personality changes which results from brain injury (in line with Paul Churchland’s theories).
In this, psychiatry struggles: while causes for mental disorders are considered medical, it is difficult to know what to examine when someone complains of mental anguish. In general, we focus on the brain—the source of what makes us us.
But ‘us’ is a conscious state of being, possibly irreducible to parts that make it function. My brain runs a continuous and self-coherent narrative—if something changes within its functioning, I may not recognise the change. I will invent my own reasons for the way things are or the way things go and I will rationalise my own decisions without external checks (just as I do not doubt the realism of my ability to fly when I’m dreaming).
A therapeutic approach which treats some specific parts of our brains cannot be easily applied or evaluated: the brain must be treated as a whole. This approach would favour talk therapy above all other interventions: a holistic approach. Yet psychiatry relies on a myriad of pharmaceuticals to alleviate mental illnesses, from anti-depressants (such as selective serotonin re-uptake inhibitors, which increase the amount of serotonin by preventing it being removed), to anti-psychotics (such as dopamine receptor-blocking drugs), which improve the patient’s wellbeing by lessening the severity and regularity of their symptoms.
Maybe we are stuck in the past. Modern psychiatric medicine has, in a way, followed in the footsteps of humorism, replacing the four humors (phlegm, black bile, yellow bile and blood) with neurotransmitters (e.g. serotonin, dopamine, norepinephrine and acetylcholine). To achieve curative effects, we attempt to strike a balance by, for example, decreasing dopamine in schizophrenia and preventing serotonin from leaving the brain in depression.
Perhaps fine-tuning the brain to the frequency of society is curative. After all, lobotomy was considered a successful intervention, leaving the patients in a numb stupor with emotional and intellectual deficits, which made them much easier to manage socially.
So, yes, the brain is not a kidney: a kidney functions in the same way in all people, whether they have 1, 2, 3 or even 4. A kidney’s function can be examined and measured, its failure can be detected and interventions may involve medications, surgery or even a transplant. A brain, however, is much more complex and a lot less understood; its physicality is more difficult to study and observations of its pathologies are much more subtle, especially with respect to mentality.
A time and a place
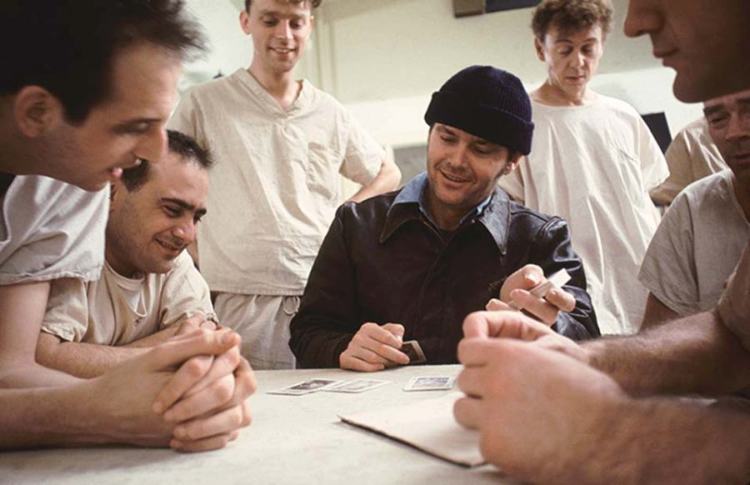
One Flew Over the Cuckoo's Nest (1975) is a film adaptation of Ken Kesey's novel by the same name in which Randle McMurphy (portrayed by Jack Nicholson), a convicted offender, is sent to a mental institution after he pleads insanity in court, expecting his time to be served in comparative luxury instead of at a prison work camp. Though the audience is told he is not mentally ill, his behaviour is seen as profoundly pathological by the staff at the institution and their therapeutic interventions intensify as his rebellion against them does too, eventually destroying them all.
Insanity and madness are common terms which are used to describe behaviour which violates social norms. As social norms have changed over time, what we observe to be disordered conduct has changed too.
Let’s think of this in practical terms: connectedness through our phones and the Internet means we get bad news fast and frequently, and the change from production-based to service-based industries means we spend more time communicating with others and more time socialising. The norm of the 9-5 work, 5 days on to 2 off, demands a constant performance which frequently spills past the 40 hours per week and finds reprieve in the structures of social pressures of procreation, visibility, beauty standards and constant advertising. As the demands for our attention increase, our time to reflect decreases, and our lives are spent in each other’s eyes through social media and in continuous communication.
There is little room for originality in this ongoing choreography: a step away from the norm is quickly noticed, and increasingly easy to discuss. A diagnosis of mental illness is quicker to acquire than it is to lose, partly because recovery is difficult to observe and partly because diagnoses in psychiatry are frequently multifold. This has been noticed by the likes of Michel Foucault and Giles Deleuze, who associated themselves with the anti-psychiatric movement. The supporters of this movement argue that psychiatric interventions are more damaging than helpful and psychiatric diagnosis is too subjective. They also protest against involuntary commitment and (what they deem to be) dangerous treatments.
Famously, psychologist David Rosenhan conducted an experiment which was published in 1973 under the title ‘On Being Sane in Insane Places’. Eight researchers feigned auditory hallucinations to gain admission into psychiatric hospitals, then behaved as they usually would from point of admission. Each was admitted on the diagnosis of ‘schizophrenia’ and discharged between 7 and 52 days later (the average stay was 19 days) with diagnosis of ‘schizophrenia in remission’. None were suspected of feigning illness by the staff, but most were suspected of feigning illness by other patients. Rosenhan concluded:
What it means to be defined

In Brave New World, a novel by Aldous Huxley published in 1932, citizens are engineered. Gestated in artificial wombs, their intelligence and future service to society is manipulated by amending the amount of oxygen and nutrients given to them as they develop. The population is kept peaceful and content using pharmaceutical interventions: there is no pain, there is only design.
Though philosophers have hypothesised and discussed how the mind works, where ‘we’ are stored in the body and what is ‘the soul’, we can imagine that their discussions and exposure to mental health and the variability in human cognition and functioning was limited. Did Immanuel Kant ever feel his heart palpitate before addressing a large crowd to a point of fainting? Did Plato ever feel the misery of doing a pile of laundry over and over again and never feeling like it got to the end? Did Isaac Newton ever ponder what the mundanity of life and constant shortages in food, warmth and rest really mean for his chambermaid?
Our brains define us, and we define our brains, in a seesaw motion, throughout our lives. Our genetic predispositions are coupled with environmental factors to give rise to who we are and who we become over time. We face moments which are great and moments which are difficult to bear; we climb to our highs and sink to our lows. Our behaviour, and the perception of our behaviour, informs the world around us who we are.
In this way, we define each other. While I cannot know if I ever was a foetus (or who I will be at the end of my life), I am pretty sure you were (and you will be you at the end of your life); to me, you persist through time. I am not privy to your inner world and you are not privy to mine: this interpersonal limitation, coupled with each individual’s uniqueness, is why psychiatry is anything but trivial.